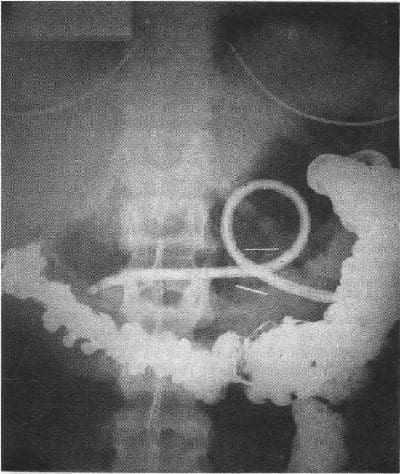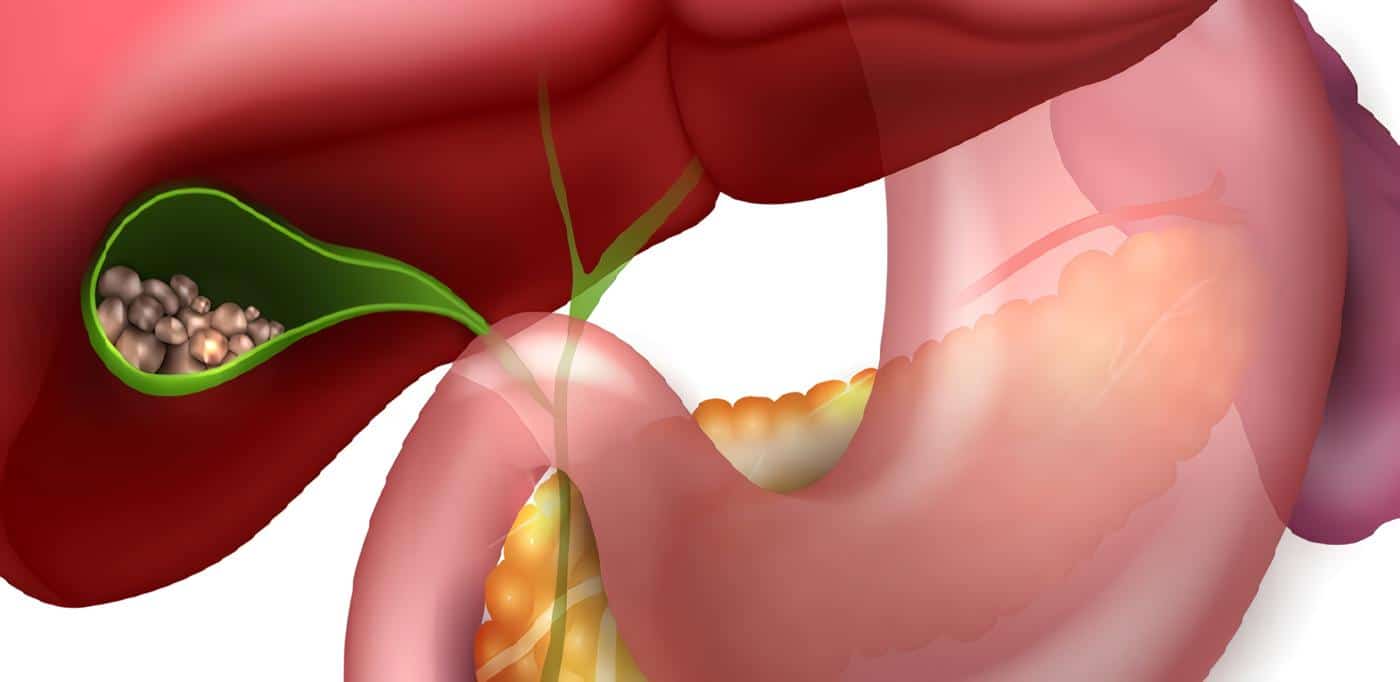
Cálculos de Colédoco
En la actualidad el endoscopista cuenta con diferentes métodos diagnósticos para detectar cálculos biliares o cálculos de colédoco.
La visualización del colédoco por ultrasonido abdominal es limitada. La TAC permite valorar el árbol biliar pero ha demostrado limitaciones para detectar los cálculos del colédoco.
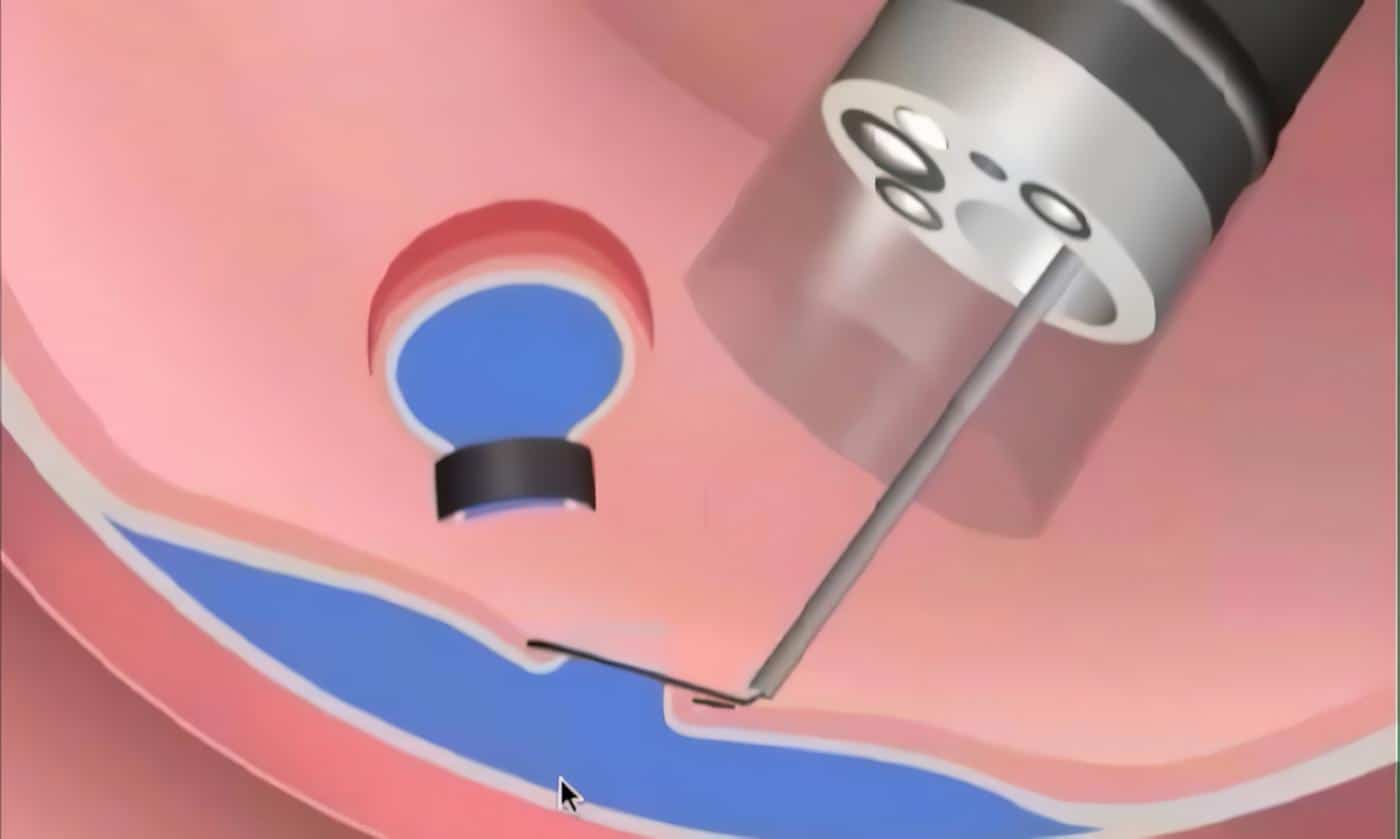
La CPRE ha sido el patrón de oro como método de alto valor diagnostico de coledocolitiasis, sin embargo, presenta riesgos importantes para los pacientes.
La EUS ha demostrado en los estudios que es una técnica sensible y específica para detectar coledocolitiasis demostrando un valor similar que los encontrados con la CPRE. Sin embargo la EUS permite ver la microlitiasis que la CPRE convencional no logra valorar adecuadamente.
Otra ventaja de la EUS es que no presenta riesgos diferentes de los de la endoscopia diagnóstica convencional (34-36). Tablas 8-9.
TABLA 8.
Valor diagnóstico de la EUS en coledocolitiasis
AUTOR |
N |
Cálculos Colédoco |
Se% |
Sp% |
Precisión % |
|
|
Edmundowicz Denis Publicidad |
(1992) |
20 |
(20%) |
75 |
100 |
95 Publicidad |
TABLA 9.
EUS en la litiasis de la VBP.
Resultados comparativos ERCP/EUS
n |
Sen |
Esp |
VPP |
VPN |
||
|
Edmundowicz 1992 Prat 1995 |
20 109 |
75% 87% |
100% 100% |
100% 100% |
93% 80% |
CPRE CPRE |
- Embarazo con US negativo
- Alergia a medios de contraste
- ERCP fallida
- Trastorno de coagulación
- ERCP dudosa
- Microlitiasis
Valor de la EUS en Coledocolitiasis
- Procedimiento altamente sensible y específico
- Mejor que US y CT
- Semejante a CPRE
- Seguro
- No exposición a Rx
- No utiliza medio de contraste
- Si demuestra tumor permite determinar su extensión
- Elige paciente para esfinterotomía
- Estudio de Pancreatitis idiopática (Microlitiasis).
EUS y Cáncer Colorectal
De acuerdo los estudios comparativos realizados entre las diferentes técnicas diagnósticas, se concluye que la USE es la mejor para estadificación del cáncer rectal tanto en sensibilidad como en especificidad.
La EUS tiene notable importancia clínica en el cáncer por la variedad de opciones terapéuticas dependientes del estado tumoral.
La EUS detecta las recidivas locales siendo utilizada como técnica de vigilancia después de tratamiento (37-40). TABLA 10.
TABLA 10.
EUS vs. TAC en la determinación del estado
local del cáncer de recto
Estado T |
Estado N |
||||
N |
EUS % |
TAC % |
EUS % |
TAC % |
|
|
Akasu |
41 |
80 |
46 |
78 |
66 |
Referencias
- 1. Rosch T, Classen M. Gastroenterologic endosonography Stuttgart Thieme, 1992.
- 2. E.S.G.E. Endoscopic Ultrasonography Endoscopy supplement 1 Vol 30, 1998.
- 3. Allgayer H, Gugler R. Usefuness and cost savings of early endoscopic ultrasound (EUS) in patients with unclear upper Gl-Wall impressions. Gastroenterology 1993; 104: 383 A.
- 4. Armengol-Miro JR, Benjamin S, et al. Clinical applications of endoscopic ultrasonography in gastroenterology. State of the art 1993. Results of a consensus conference, Orlando Florida, january, Endoscopy 1993; 25: 358-366.
- 5. Boyce GA, Sivac MV, Rosch T, et al. Evaluation of submucosal upper gastrointestinal tract lesions by endoscopic ultrasound. Gastrointest Endosc 1991; 37: 449-454.
- 6. D Vroak H, Zavoral M. Submucosal tumors of the upper gastrointestinal tract: Diagnosis by Endoscopic Ultrasonography. Endoscopy 1994; 26: 823 Abstract.
- 7. Dittler HJ, Siewert JR. Role of endoscopic ultrasonography in esophageal carcinoma. Endoscopy, 1993; 25: 156-61.
- 8. Ginsberg CG, AL-Kawas FH, Nguyenne CC, et al. Endoscopic ultrasound evaluation of vascular involvement in esophageal cancer: A comparison with computer tomography. Gastrointest endosc 1993; 39: A 276 Abstract.
- 9. Wiersema MJ, Vilman P, Gionanini M, et al. Endosonography guided fine nedle aspiration biopsy: Diagnostic accurasy and complication assessment. Gastroenterology 1997; 112: 1087-95.
- 10. Callimanis GE, Gupta PK, AL Kawas FH et al. Endoscopic ultrasound for staging esophageal cancer, with or without dilation, is clinically important and safe. Gastrointest Endosc 1995; 41: 540-6.
- 11. Chak A, Canto M, Gerdes H, et al. Prognosis of esophageal cancers preoperatively stage to be locally invasive (T4) by endoscopic ultrasound (EUS): A multicenter retrospective cohort estudy. Gastrointest Endosc 1995; 42: 501-6.
- 12. Giovannini M, Seitz JF, Thomas P, et al. Endoscopic Ultrasonography for assessment of the response to combined radiation therapy and chemotherapy in patient with esophageal cancer. Endoscopy 1997; 29: 4-9.
Bibliografía
- 13. Van Damme J, Falk GW, Sivac MV, et al. Endosonographic evaluation of the patient with achalasia: Apperance of the esophagus using the ecoendoscope. Endoscopy 1995; 27: 185-90.
- 14. Schiano TD, Fischer RS, et al. Use of high – resolution ultrasonography to assess esophageal wall damage after pneumatic dilation and botulinum toxin injection to treat achalasia. Gastrointest Endosc 1996; 44: 151-7.
- 15. Hoffman BJ, Knapple WL, Bhutani NS, et al. Treatment of achalasia by injection of botulinum toxin under endoscopic ultrasound guidance. Gastrointest Endosc 1997; 45: 77-9.
- 16. Nakamura H, Inowe H, Kawano T, et al. Selection of the treatment for esofagogastric varices. Analyses of colateral estructures by endoscopic ultrasonography. Surg Endosc 1992; 6: 228-234.
17. Grimm H, Binmoeller KF, Hampr K, et al. Endosonography for preoperative locorregional stageing of esophageal and gastric cancer. Endoscopy 1993; 25: 224-30. - 18. Akahoshi K, Misawa T, Fugishima H, et al. Preoperative evaluation of gastric cancer by endoscopic ultrasound. Gut 1991; 32: 479-82.
- 19. Tio TL, Kallimanis GE. Endoscopic ultrasonography of perigastrointestinal lymph nodes. Endoscopy 1994; 26: 776-9.
- 20. Caletti G, Ferrari F, Brocchi E, et al. Accuracy of endoscopic ultrasonography in the diagnosis and staging of gastric cancer and Lymphoma. Surgery 1993; 113: 14-27.
- 21. Takemoto T, Tada M, Dittler HJ, et al. lmpact of staging on treatment of gastric carcinoma. Endoscopy 1993; 25: 46-50.
- 22. Chonan A, Mochizuki F, lkeda T et al. Endoscopic ultrasonography for the diagnosis of malignant lymphoma of the estomac. Gastroenterol Endosc 1992; 1833-43.
- 23. Caletti GC, Bocus, Roda E. Endoscopic ultrasonography in primary gastric lymphoma. lN: Morton A. Meyers, editor. Neoplasms of the digestive tract: lmaging, staging and management. Philadelphia: Lippincott-Raven, 1998; 157-63.
Fuentes
- 24. Mendis RE, Gerdes H, Lighdale CJ, Botet JF. Large gastric folds: A diagnostic approach using endoscopic ultrasonography. Gastrointest Endosc 1994; 40: 437-41.
- 25. Rosch T. Staging of pancreatic cancer analysis of literature results. Gastrointest Clin N Am 1995; 5: 735-9.
- 26. Yasuda K, Mukai H et al. Staging of pancreatic cancer by endoscopic ultrasonography. Endoscopy 1993; 25: 151-5.
- 27. Brugge WR. Pancreatic cancer staging: Endoscopic ultrasonography criteria for vascular invasion. Gastrointest Endosc N Clin Am 1995; 5: 741-53.
- 28. Chang KJ, Nguyen P, Erickson RA, et al. The clinical utility of endoscopic ultrasound-guided fine needle aspiration in the diagnosis and staging of pancreatic carcinoma.. Gastrointest endosc 1977; 45: 387-93.
- 29. Rosh T, Lorenz R, Neuhaus H et al. The value of endoscopic ultrasound in chronic pancreatitis. Gastrointest Endosc 1991; 37: 254-5.
- 30. Lees WR. Endoscopic Ultrasonography of chronic pancreatitis and pancreatic pseudocyst. Scand J Gastroenterol 1986; 21(supp 123): 119-22.
- 31. Mukei H, Yasuda K, Nakajima M. Tumor of the papilla and distal common bile duct: Diagnosis and staging by endoscopic ultrasonography. Gastrointest Endosc Clin N Am 1995; 5: 763-72.
- 32. Tio TL, Sie H, Kallimanis G et al. Staging of ampulary and pancreatic carcinoma: Comparison between endosonography and surgery. Gastrointestinal Endosc 1996; 44: 706-13.
- 33. ltoh A, Goto H, Naitoh Y et al. lntraductal ultrasonography in diagnosing tumor extension of cancer of the papila of Vater. Gastrointest Endosc 1997; 45: 251-60.
- 34. Edmundowicz SA et al. A prospective comparison of endoscopic ultrasound, ERCP, and standard abdominal ultrasonography for the detection of choledocholithiasis prior tolaparoscopic cholecystectomy. Gastrointest Endoscopy 1994; 40: 63. A193.
- 35. Edmundowicz SA. Choledocholithiasis. Gastrointest Endosc N Clin Am 1995; 5: 791-97.
Lecturas Recomendadas
- 36. Prat F, Amouyal G, Amouyal P, et al. Prospective controlled study of endoscopic ultrasonography in patients with suspected common bile duct lithiasis. Lancet 1996; 347: 75-9.
- 37. Herzog U, Von Flue M, Tondelli P, Schuppiser JP. How accurate is endorectal ultrasound in the preoperative staging of rectal cancer. Dis Colon Rectum 1993; 36: 127-34.
- 38. Williamson PR, Hellinger MD, Larach SW Ferrara A. Endorectal ultrasound of T3 and T4 rectal cancers after preoperative chemoradiation. Dis Colon Rectum 1996; 39: 45-9.
- 39. Kahn H, Alexander A et al. Preoperative staging of irradiated rectal cancers using digital restal examination, computed tomography, endorectal ultrasound and magnetic resonance imaging does not accurately predict TONO pathology. Dis Colon Rectum 1997; 40: 140-4.
- 40. Romano G, Belli G, et al. Colorectal cancer. Gastrointest Endosc N Clin Am 1995; 5: 805-14.