Quizás fue Galeno (130-210 D.J.), quien alejándose de los preceptos hipocráticos, que consideraban la tisis como una enfermedad hereditaria, se refirió a los peligros que entraña el contacto próximo con esos enfermos. La naturaleza hereditaria proclamada por Hipócrates perdura hasta comienzos del siglo XVI en que Fracastoro de Verona se refiere a la naturaleza contagiosa de la enfermedad.
El Consejo Sanitario de Florencia en 1753 elabora un proyecto de ley para combatir la “plaga blanca” de la cual se asegura es contagiosa, ya que “el enfermo al toser desprende pequeñas partículas impuras que causan la enfermedad a las personas que la rodean”.
A finales el siglo XVI los tuberculosos de los países de Europa meridional estaban desposeídos de derechos como los leprosos en la edad media. Disponían de hospitales propios donde los pobres eran acogidos gratuitamente. Pero todo el mundo sentía horror ante la posibilidad de ingresar en dichos sanatorios, pues allí no se podría esperar otra cosa que la muerte. (Lea también: La Tuberculosis, Los Cambios Acontecidos en el Modelo Clínico de la Enfermedad)
El descubrimiento del M. tuberculosis por Koch en 1882 y el conocimiento del contagio de la enfermedad llevaron racionalmente a la idea de aislar a los enfermos en hospitales especiales o sanatorios donde se les internaba a menudo por períodos muy largos.
Estas instituciones estaban ubicadas generalmente en el campo, a la orilla del mar o en las montañas, ya que el aire era considerado como benéfico para estos pacientes y necesario para su recuperación.
En Colombia la primera referencia oficial en materia preventiva fue hecha por la Junta Central de Higiene en 1896 (35), la cual ordenó aislamiento de las personas que según criterio médico padecieran de tuberculosis, siempre que se hallasen recluidas en pensiones o en cuarteles. La Ley 66 de 1916 ordena el funcionamiento de pabellones especiales para el aislamiento de tuberculosos en los hospitales generales y en las cárceles.
En 1942 se funda el Hospital Antituberculoso Santa Clara de Bogotá. En 1949 se construye el Hospital San Carlos también en Bogotá, dedicado igualmente al aislamiento y cuidado del paciente tuberculoso. Posteriormente se edifican numerosos sanatorios a través del territorio nacional.
El descubrimiento de la estreptomicina en 1943 y luego del resto de las drogas antituberculosas que demuestran un magnífico resultado frente la infección tuberculosa llevan al Manifiesto de Madrás en 1959 (37) cuando se definió que “los pacientes tuberculosos tratados adecuadamente en forma ambulatoria se curan en un 100% sin necesidad de hospitalización, excepto los casos de extrema gravedad que por su estado general de salud lo requieran”.
El resurgimiento de la tuberculosis, especialmente en los países desarrollados, el aumento en la prevalencia de cepas de M. tuberculosis resistente a las drogas conocidas, la discontinuidad y falla de control de los pacientes tuberculosos y las fatales consecuencias del creciente número de asociaciones de TB-SIDA ha movido a las entidades gubernamentales de salud de países como los Estados Unidos (11, 30, 42, 43, 120) a recomendar, de nuevo, la reclusión de los enfermos para una adecuada supervisión de los tratamientos, un mejor cuidado de ellos así como de la población que los rodea, susceptible de ser contagiada.
Capítulo 12. Obscuras perspectivas, que con Justificada razón, se vislumbran sobre el aumento de incidencia de la tuberculosis, enfermedad modificada, que amenaza en convertirse otra vez, en una plaga para la humanidad
El hecho de que Colombia haya seguido siendo un país con una alta incidencia de tuberculosis, de que su tasa de salubridad corresponda a la de un país en vías de desarrollo y que su incidencia de SIDA esté en aumento, presupone un mal pronóstico para el futuro de la epidemiología y control de la tuberculosis en el país, en los años venideros.
Recapitulando y volviendo sobre datos ya anotados recordemos que la incidencia de tuberculosis es en Colombia aproximadamente de 32 por 100.000, su prevalecencia de 170 por 100.000 y el riesgo de desarrollar la enfermedad en pacientes infectados, de 2 a 5% (20 a 25 veces mayor que en los países desarrollados). Las cifras anotadas sólo corresponden aproximadamente a la tercera parte de la realidad.
El número de casos de SIDA es nuestro país hasta el presente año es de 3.304 casos y de 2.855 el número de personas infectadas por el VIH; calculándose un subregistro del 90%.
Se calcula que para el año 2000 habrá en el mundo 10millones de enfermos y 40 millones de individuos infectados (con un subregistro de infectados del 90%y de enfermos del 70%).
Un 30 a 50%de los pacientes infectados por el VIH presentan tuberculosis concomitantemente.
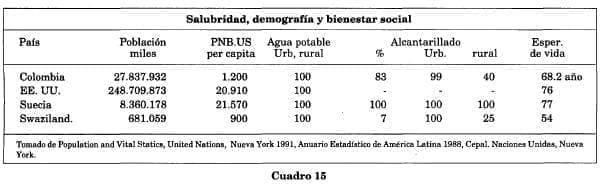
Las condiciones sanitarias de nuestro país distan mucho de ser las mejores (Cuadros 15 y 15A), el hacinamiento en las grandes ciudades por inmigración de los campesinos que huyen de la violencia de los campos y la falta de protección en sus pueblos, la desnutrición, el consumo indebido de drogas, la dureza del trabajo y el poco tiempo dedicado al descanso, todo esto disminuye la resistencia del individuo a la infección y aumentan los riesgos de padecer la enfermedad.

La incidencia de la tuberculosis disminuyó en el mundo industrial gracias al mejoramiento del nivel de vida, de la atención médica y de los programas preventivos de salud. En cambio, persistió en los países del tercer mundo, donde sigue siendo un grave problema de salud pública por subsistir las bajas condiciones de vida de los años que precedieron a la revolución industrial en Europa y los Estados Unidos.
Si bien es cierto que la quimioterapia específica contra la tuberculosis constituyó casi una panacea para la curación de la enfermedad, la aparición de cepas resistentes a estas drogas, la demora en su reconocimiento, la falta de aislamiento conveniente de los enfermos que la presentaban, la falla en el control de su tratamiento, han dado lugar a una menor respuesta a la terapia, un mayor rechazo del Micobácterioa la droga y a una mayor diseminación de la enfermedad.
Todos estos factores aunados podrían explicar el aumento en la incidencia entre nosotros y en el mundo entero de la tuberculosis que amenaza, como ya se ha dicho repetidamente, con convertirse en una nueva plaga para la humanidad.
Su control significa organizar un programa multifacético en el cual debe estar empeñado el orbe entero.
Para terminar vale la pena recalcar que el objetivo de esta presentación, como ya se advirtió al comienzo del estudio, es poner en alerta a los especialistas en ortopedia ante la reaparición en Colombia, y en el mundo, de la tuberculosis, una enfermedad que constituyó por muchos siglos una verdadera plaga para la sociedad.
Que fue vencida a mediados del presente siglo gracias al descubrimiento de su causa, al desarrollo de vacunas y a la aparición de drogas específicas, pero que por diferentes causas ambientales ha hecho su reaparición con un vigor que amenaza con convertir esta enfermedad, en las postrimerías del siglo XXI, en un nuevo azote para la humanidad.
El ortopedista debe pensar en esta afección en todo caso de lesión inflamatoria osteoarticular subaguda o crónica que no responda al tratamiento antiinfeccioso habitual, y llevar a cabo los exámenes más apropiados para su pronto diagnóstico y tratamiento específico.
Se debe recordar que la tuberculosis y el SIDA suelen ser compañeros inseparables. Esta última enfermedad al disminuir las defensas del huésped facilita la infección de gérmenes oportunistas y entre ellos especialmente el Micobacterium tuberculosis. La asociación de las dos entidades modifica notablemente el modelo biológico de la tuberculosis y agrava aún más su mal pronóstico.
Bibliografía
1. ABDELWAHABD I.F.; KENAN S.; HERMAN G.; LEWIS M.; KLEIN M.; RABMIOWITZ J.G.: Atypical Skeletal Tuberculosis Mimicking Neoplasm. British J. Radiol. 64: 551, 1991.
2. ALBERTS B.; BRAY D.; JEWIS J.; RAFF M.; ROBERTS K; WATSON J.D.: Molecular Biology of the ceBo2nd. Ed. GarlandPubl. Inc. NewYork, 1989.
3. ALVAREZ S.; McCABE W.R: Extrapulmonary tuberculosis: A Review of Experience at Boston City and other Hospitals: Medicine 63: 1, 1984.
4. Am. Rec. Respir. Dis. 119, 107, 1979.
5. ARANGO M.: Diagnóstico y tratamiento de la tuberculosis en el niño. Primer Seminario de Epidemiología y Control de la Tuberculosis. Ibarra, Ecuador, julio 1991.
6. AUERBACH O.: Acute generalized miliary tubercu- 10sis.Am. j. Pathol. 20: 121, 1944.
7. BARBER T.W.; CRAVEN D.E.; McCABE W.R: Bacteremia due to Mycobacterium tuberculosis in patients with ~lUman inmunodeficiency virus infections. Medicine 69, 375, 1990.
8. BARNES P.F.; BLOCH A.B.; DAVIDSON P.T.; SNIDER, D.E.:Tuberculosis in patients with Human Inmunodeficiency virus infections. N. Engl. J. Med.: 324: 1644, 1991.
9. BATUNGWANAYOJ.; TALEMAN H.; DHOTE R; BOGAERTS J.; ALLEN S. van de PERRE P.: Pulmonary Tuberculosis in Kingali, Rwanda.: Am. Rev. Respir. Dis. 146: 53, 1992.
10. BRAUN M.M.; BYERS RH.; HEYWARD W.L.; CIESIELSKI C.A., Bloch V.R, Berkelman RL., Snider D.E.: Acquired inmunodeficiency Syndrome and Extrapulmonary Tuberculosis in the United States. Arch. Intern. Med. 150, 1913, 1990.
11. BRUCE DULLH.:About the CDC.Am.J. PrevoMed. 8: 268, 1992.
12. BABHULKAR S.S.; TAYADEW.B.; BABHULKAR S.K: Atypical Spinal Tuberculosis. J. Bone Joint Surg.: 66-B: 239, 1984.
13. BAILEYH.L.;GABRIELM.;HODGSONA.R; SHIN J.S.: Tuberculosis ofthe spine in children: Operative findings and results in 100 consecutive patients treated byremoval ofthe lesion and anterior grafting. J. Bone Joint Surg.: 54-A: 1633, 1972.
14. BURKE RM.: An historial chronology of tuberculosis. Second edition. Springfield. 111.,Charles C. Thomas 1955.
15. BURROUGHS M.; EDELSON P.J.: Medical Care of the HIV-Infected Child.: PedoClin. NorthAm. 38:45, 1991.
16. CALONJE J.H.: Tuberculosis ost’=loarticular: En Bernal J.J.: La Infección Osteoarticular: 79: Universidad del Quindío, Armenia, Colombia, 1989.
17. CDC.Astrategic plan for the elimination oftuberculosis in the United States. MNWR:38 (suppl n. S-3): 1-25,1989.
18. CANETTI G.;DEBEYRE J. Y SEZE S.: Stérilisation des lésions de la tuberculose ostéo-articulaire par la chimiothérapie antibacillarie. Rev. de la Tub. (Paris) 5a. serie. 21: 1337, 1957.
19. CANETTI G.; FOX W.; KHOMENKO A. et al.: Advances in techniques of testing mycobacterial drug sensitibity and the use of sensitibity tests in tuberculosis control programmes. Bull. WHO41: 21. 1969.
20. CANO C.; VILLAREAL C.; GOMEZ A.; RAMIREZ F., BECERRA G.: La importancia de la tuberculosis en el síndrome de Inmunodeficiencia adquirida. Aspectos clínicos y terapéuticos. Gazeta Médica de Méjico: 127: 2,137,1991.
21. CATHEBRAS P.; VOHITO J.A.; YETA M.L. et al.: HIV infection among patients with tuberculosis in Bailgui (Central African Republic): a prospective study. Xllth International Congress for Tropical Medicine and Malaria. 1988. Int. Congress Ser. 810: 66,1988.
22. CICERO-SABIDO R: Pott’s Disease. Letter to the Editor. Chest 96: 955, 1989.
23. CORDERO M.; SANCHEZ I.: Brucellar andtuberculous spondylitis J. Bone Joint Surg.: 73-B: 100,1991.
24. CRAMERK.;GRAYS.J.; MILEKM.A.: Tuberculous ofthe wrist, Two cases reporto Clin. Orth: 262: 137, 1991.
25. CHAPMAN C.B.; WHORTEN C.M.: Acute generalized tuberculosis in adults. N. Engl. J. Med. 235: 2398, 1946.
26. CLARKRA; BLAKLEY S.L.; GREER D.; SMITH M.H.D.; BRANDON W.; WISNIESWSKI T.L.: Hematogeneous Dissemination of Mycobacterium tuberculosis in Patients with AIDS. Rev. Infect. Dis. 13: 1089, 1991.
27. CHRETIEN J.: Tuberculosis y VIH. El dúo maldito. Bull. Int. Tuberc. Lung. Dis. 65: 27, 1990.
28. DALEY Ch.; SMALL P.A.; SCHECTER G.F.; SCHOLNIK G.K.; McADAMRM.; JACOBS W.R; HOPEWELL P.C.:An Outbreak oftuberculosis with Acelerated Progression among persons infected with Human imunodeficiency virus. N. Engl. J. Med. 326, 231,1992.
29. Diagnosis and Treatment of disease by ‘non tuberculous Mycobacteria. Am. Rev. Respir. Dis. 142, 940, 1990.
30. DOOLEY S.W.; JARVIS W.R; MATONE W.J.; SINIDEER D.E.: Multidrug resistant Tuberculosis (Editorial). Ann. Int. Med. 117,257, 1992.
31. DAVIDSONP.T.; HOROWITZ l.: Skeletal tuberculosis: A Review with Patients Presentation and discussion. Am. J. Med.: 487: 77, 1970.
32. DEBEAUMONT A: Bactériologie de la tuberculose ostéo-articulaire sous chimiothérapie. Adv. Tuberc. Res. 15: 125, 1966.
33. East African and British Medical Research Council co-operative investigation. Tuberculosis in Kenia. A second national sampling survey of grug reistance and other factors, and comparison with the prevalence data from the first national sampling survey. Tubercle 59: 155, 1978.
34. Editorial: Tuberculosis ofthe Spine. Lancet: 2: 137, 1974.
35. ERASO C.L.: Historia de la tuberculosis. Primer seminario de Epidemiología y Control de la tuberculosis. Ibarra, Ecuador, Julio 1991.
36. ENARSON D.A: Pott’s Disease: Letter to the Editor. Chest 96: 955, 1989.
37. Experiencias de Madrás. British Council for TBC Reasearch 1960.
38. FANG D.; LEONG J.C.Y.; FANG H.S.Y.: Tuberculosis ofthe upper cervical spine. J. Bone Joint Surg.: 65-B: 47,1983.
39. FANNING A; DIERICH H.; LENTLE B.: Bone Scanning with Technetium 99m Tc Polyphosphate in tuberculous osteomyelitis. Tubercle: 55, 227, 1974.
40. FARER L.S.; LOWELL A.M.; MEADOR M.P.: Extrapulmonary tuberculosis in the United States. A J. Epidemiology. 109: 205, 1979.
41. FERRERX.; KIRSCHBAUMA; TOROJ.; JADIN J.; MUÑOZ N.; ESPINOZA A: Adherencia al tratamiento de la tuberculosis del adulto en Santiago de Chile. O.S.P.: 111,423, 1991.
42. FISCHL M.A.;UTTAMCHANDANIR.B.; DIAKOS G.L.;POBLETE R.B.;MORENO T.J.; REYES RR; BOOTA AM.; THOMPSON L.M.; CLEARY T.J.; LAY S.: An Outbreak of Tuberculosis Caused by Multiple-Drug-resistant Tubercle Bacilli among Patient with HIV Infection. Am. Coll. Physc. 117, 177,1992.
43. FISCHL M.A; DAIKOS G.L.; UTTAMCHANDANI RD.; POBLETE RB.; MORENOJ.N.; REYES RR; BOOTA AM.; THOMPSON L.M.; CLEARY T.J.; OLDHAM S.A.; SALDAÑA M.J.; LA! S.: Clinical Presentation and Outcome of Patients with HIV Infection and Tuberculosis Caused by Multiple-Drug resistant Bacilli. Ann. Int. Med. 117, 184, 1992.
44. GILLESPIE W.J.: Skeletal tuberculosis series chemoterapy. J. Bone Joint Surg.: 70-B, 163, 1988.
45. GOLDBERG J.; KOVARSKY J.: Tuberculosis Sacroileitis. Southern Med. J.: 76:9, 1175.
46. GLASSCHEIB H.8.: El laberinto de la Medicina: Errores y TrÍunfos de la Terapéutica. Ed. Destino. Barcelona 1964.
47. GLASSROTHJ.; ROBINS A.G.; SNIDER D.E.: Tuberculosis in the 1980s:New England J. Med.: 302: 261441
48. GLOYDS.;LOPEZJ.L.;MERCADOF.J.;DURMING J.: Riesgode infecciónpor Mycobacterium tuberculosis en Jalisco, México O.P.S.: 111, 393, 1991.
49. GOVENDER S.; CHARLES RW.: Tuberculosis of the cervical spine. J. Bone Joint Surg.: 72-B, 748, 1990.
50. GUERRA DE MACEDO, C.: Mensaje del Director: O.S.P.: 111, 193, 1991.
51. GRIFFITHS D. Ll.: Tuberculosis of the spine: a Review Adv. Tuberc. Res. 20: 92, 1980.
52. GAVILANESJ.: Introducción: Primer Seminario de Epidemiología y Control de Tuberculosis. Ibarra, Ecuador, julio 1991.
53. HECKBERT S.R; ELARTH A; NOLAN Ch. M.: Virus Infection on Tuberculosis Men in Seattle- King County, Washington. Chest 102, 433,1992.
54. HACEDWEGER S.;MILDRAND.S. et al.: Tuberculosis as a manifestation of the acquired immunodeficiency Syndrome. JAMA: 256, 362, 1986.
55. HALSEY J.P.; REEBACK J.S.; BARNES C.G.: A decade ofskeletal tuberculosis. Ann Rheum. Dis. 41: 7,1982.
56. HARDINGE K; CLEARYJ.; CHARNLEYJ.: Lowfriction artroplasty for healed septic and tuberculous arthritis. Journ. Bone Joint Surg.: 610B: 144, 1979.
57. HARDINGE K.; WILLIAMS D.; ETIENNE A; MacKENZIE D.;CHARNLEYJ.: Conversion offused hips to low friction artroplasty. J. Bone Joint Surg.: 59-B: 385, 1977.
58. HARRIS A.D.: Tuberculosis and Human Immunodeficiency virus infection in developingcountries. Lancet 335: 8686, 1990.
59. HECHT R.H.; MEYERS M.H.; THORNEHILLJOYNES M.; MONTGOMERIR J.: Reactivation of tuberculous infection following total joint replacement. J. Bone Joint Surg.: 1015, 1983.
60. HENRIQUES C.Q.: Osteomyelitis as a complication in urologyWith special reference to the paravertebral venous plexus British J. Surg.: 19, 1958.
61. HODGSON, AR; STOCKF.E.; FANGH.S., y ONG G.B.:Anterior spinal fusion: the operation approach an pathological findings in 412 patients with Pott’s disease ofthe spine. British J. Surg.: 48: 172, 1960.
62. HODGSON,AR;STOCKF.E.:Anteriorspinefusion for the treatment of tuberculosis of the spine. The operative findings and results of treatment in the first one hundred cases. J. Bone Joint Surg.: 42-A: 295,1960.
63. HOLDER S.; HOPSON C.; VONKUSTER L.C.: Tuberculous Arthritis ofelbowpresenting as chronice bursitis ofthe olecranon. J. Bone Joint Surg.: 67-A: 1127,1985.
64. HSU L.C.; CHENG C.L.: Pott’s paraplegia of late onset: recovery after anterior decompression. J. Bone Joint Surg.: 68-B: 676, 1986.
65. HSU L.C.S. y LEONG J.C.Y.: Tuberculosis of the lower cervical spine (C2to C7):AReport of40 Cases.: J. Bone Jonint Surg.: 66-B: 1, 1984.
66. JANSEN RS.; et al.: HIV Infection among patients in USoAcute Care Hospitals. New Engl. J. Med. 327, 445,1992.
67. JOHSON R; BARNESK.L.;OWENR: Reactivation oftuberculosis after total hip Replacement: J. Bone Jóint Surg.: 61-B: 148, 1979.
68. KeniaIBritish Medical Research Council co-operative investigation. Tuberculosis in Kenia 1984: a third national survey and comparison with earlier surveys in 1964 and 1974,. Tubercle; 70:5, 1989.
69. KEY J.A: Positive Pressure in Arthrodesis for Tuberculosis ofthe kneejoint. South Med. J.: 25: 909, 1932.
70. KIMYOUNG-HOO;HANDAE-YONG;PARKB.M.: Total hip arthroplasty for tuberculous coxarthrotis. J. Bone Joint Surg.: 69-A: 5, 718.
71. KONSTAM, P.G. y KONSTAM, S. T.: Spinal tuberculosis in southern Nigeria. With special reference to ambulant treatment ofthoracolumbar disease. J. Bone Joint Surg.: 40-B: 26, 1958.
72. KONSTAM,P.G. y BLESVOSKYA: The ambulant treatmentofspinal tuberculosis. BritishJ. Surg.: 50: 26,1962.
73. KUMAR K.; SAXENA M.B.L.: Multifocal osteoarticular tuberculosis. Int. Orthopaedics: 12: 135,1988.
74. LA BERGE J.M.; BRONDT-ZAWADZKI M.: Evaluations of Pott’s disease with Computedtomography. Neuroradiology: 26: 429,1984.
75. LACHENAUER C.S.; COSENTINO S.;WOODRS. et al.: Multifocal skeletal tuberculosis presenting as osteomyelitis ofthe jaw. Pediatr. Infect. Dis. J.: 10: 940,1991.
76. LAIN-ENTRALGOP.ycol.: Historia Universal de la Medicina. Salvat Ed. Barcelona 1974.
77. LEVI G.C.; MENDES W.S.; RODRIGUEZ G.A.;et al.: Tuberculosis (TB and acquired immunodeficiency syndrome (AIDS), XIIth International Congress for Tropical Medicine and Malaria. Int. Congress Ser 810: 66 1988.
78. LE ROUX; GRIFFIN G.E.; MORSCH H.T; WINN R: Tuberculosis ofthe skul1:Arare condition: Case Report and Review ofthe literature. Neurosurgery 26: 5, 851.
79. LIN-GREENBERG A Y CHOLANKERIL J.: Vertebral Arch Destruction in Tuberculosis. J. Computer Assited Tomography: 14 (2): 300, 1990.
80. LIFESO R.M.; WEAVER P.; HARDER E.H.: Tuberculous Spondylitis in Adults. J. Bone Joint Surg.: 67-A: 1504, 1985.
81. LIFESO R: Atlanto-axial tuberculosis in adults. J. Bone Joint Surg.: 69-B: 183, 1987.
82. LUDMERER K; KISSANE J.M.: Severe Right hip Pain in a 73 year old woman. Clinico-pathologic Conference. Am. J. Med. 81: 117, 1986.
83. McTAMMANYJ.R; MOSER KM.; HOUK V.N.: Disseminated bone tuberculosis. Am. Rev. Resp. Dis.: 87, 1889, 1963.
84. MAIER W.P.; WILMER Ch. 1.; WILSON C.H.: Meningitis Associated with tuberculous arthritis of the knee. Am. J. Med.: 80: 151, 1986.
85. MALAGONV. y ARANGO R: Ortopedia Infantil. Editorial JIMS Barcelona 1987.
86. MALAGONV.: Contribución al estudio del Mal de Pott en el niño. Tesis de Grado. Universidad Nacional de Colombia. Bogotá, 1950.
87. MALAGON V.: Tuberculosis espinal en el niño: Revisión de 63 enfermos. Medicina. 3, 11, 1979.
88. MALAGON V.: Tuberculosis osteoarticular. Rev. Ped.]JCXl: 1. 1978.
89. MANNJ.S.; COLE RB.: Tuberculous spondylitis in the elderly a potential diagnostic pitfall. Bristish Med. J.: 2947, 1149, 1987.
90. MANN J.; SNIDER D.; FRANCIS H. et al.: Association between HTLV-IIVLAVinfection and tuberculosis in Zaire. JAMA 256: 346, 1986.
91. Medical Research Council Working Party on Tuberculosis ofthe spine:AControl1edtrial ofambulant outpatient treatment and impatient rest in bed in the mangement of tuberculosis of the spine in patients on standard chemotherapy. J. Bone Joint Surg.: 55-B: 678, 1973.
92. Medical Research Council Working Party on Tuberculosis treatment of the Spine: Second Report. A Control1ed trial of Plastic-of-Paris Jackets in the Management of Ambulant Outpatient Treated of Tuberculosis of the Spine in Children on Standard Chemotherapy: AStudy in Pusam, Korea: Tubercle: 54: 261, 1973.
93. Medical Research Council Working Party on Tuberculosis treatment ofthe Spine: A control1ed trial of anterior fusion and débridement in the surgical management oftuberculosis ofthe spine in patients on standard chemotherapy: a study in Hong Kong,: British J. Surg.: 61: 853, 1974.
94. Medical Research Council Working Party on Tuberculosis ofthe Spine: Acontrol1ed trial ofanterior spinal fusion and débridement in the surgical management oftuberculosis ofthe spine in patients on standard chemotherapy: A study in two centres in South Africa.: Tubercle 59: 79, 1978.
95. Medical Research Council Working Party on Tuberculosis of the Spine. A control1ed trial of sixmonth and nine-month regimens of chemotherapy in patients undergoing radical surgery for tuberculosis of the spine in Hong Kong: Tubercle 67: 243, 1986.
96. MedicalResearch CouncilWorkingParty onTuberculosis of the spine. A 10-year assesment of control1ed trials of in patient and out patient treatment and of Plaster-of-Paris J ackets for tuberculosis ofthe spine in children on standard chemotherapy.
97. Medicine 49: 243, 1970.
98. M.M.W.R: Centers for Disease Control: 36: 50 & 51, 1988.
99. M.M.W.R: Centers for Disease Control: 39/No. RR- 8: 1, 1990.
100.M.M.W.R: Center for Diseases Control. Tuberculosis. Final Data. United States, 1986,36: 817,1988.
101.M.M.W.R: Center for Diseases Control 36 (Suppl.): ls-15s, 1987.
102.MARTINI M.; ADJRAD A; BOUDJEMAA A: Tuberculosis osteomyelitis Int. Orthopaedics: 20: 201, 1986.
103.MATAMOROSC.: Infecciones de la columna vertebral: En Bernal J J: La infección osteoarticular. 115: Universidad del Quindío, Armenia, Colombia 1989.
104.Ministerio de Salud: Subdirección Control de Patología. División Patologías transmisibles. Programa Control tuberculosis, mayo 1993.
105. Ministerio de Salud: Programa de ETSNIH/SIDA Informe parcial. Mayo 1993.
106. MULERO J.; ANDREU J.L.: Inflamación articular: Formación Médica Continuada: Europharma 1991.
107. MOSS W.J.; DEDYOT.; SUAREZM.;MICHOLAS S.W.;ABRAMSE.: Tuberculosis in children infected with human immunodeficiency virus: A report of five cases. Pediatr. Infect. Dis. J.: ll: 114, 1992.
108. NAMBUYAA.; SEWANKA.MBON.; MUGERWA J.; GOODGAME R.; LUCAS S.: Tuberculous lymphadenitis associated with human immunodeficiency virus (HIV) in Uganda. J. Clin. Pathol. 41: 93,1988.
109. NARVAEZ O.:Métodos de diagnósitco en Tuberculosis según el Programa. Primer Seminario de Epidemiología y Control de Tuberculosis. Ibarra, Ecuador, julio 1991.
110. NAVASG.: Comunicación personal.
111. N. Engl. J. Med.: 328, 1007, 1993.
112. NOEL G.J.: Host Defense Abnormalities Associated with HIV Infection. Pedo Clin. North Am. 38: 37, 1991.
113. OCHOA L.C.: Seccional de Salud de Antioquia. Comunicación del 6 de mayo de 1993.
114. OMARIB.; ROBERTSON J.; NELSON RJ.: Pott’s Disease: A Resurgent Challenge to the thoracic Surgeon. Chest: 95: 145, 1989.
115. OROZCO L.C.: Comunicación personal.
116. PACHECO L.A.; MENDEZ V.; ESPINEL R.; MALAGON V.: Tuberculosis espinal en el niño. Hospital Infantil de Bogotá, 1975.
117. PINZON A.: Tuberculosis en poblaciones de Territorios Nacionales de Colombia. Incidencia de la Población Indígena Medicina: 16: 49, 1987.
118. PITCHENIKA.E.;COLEC.;RUSSELLB.W.atal.: Tuberculosis atypical micobacteriosis and the adquiere inmunodeficiency syndrome among traite sis and no traitiasis patients in South Florida. Ann. Intern. Med. 101: 645, 1984. Ann. Intern. Med.: 106: 254: 1987.
118-A.PITCHENIKA.E.; RUSSELLB.W.; CLEARYT.; PEJOVIC l.; COLE C.; SNIDER D.E.Jr.: The prevalence of Tuberculosisand drug resistance among Haitians . N. Engl J. Med. 307: 162, 1982.
119. POUCHOT J.; VINANEUX P.; BARGE J.; BOUSSOUUGAUT Y.; GROSSIN M. PIERRE J.; CARBONC.;KAHNM.F.; ESCAILEJ.M.: Tuberculosis of the Sacroiliac Joint: Clinical. Feature. Outcome and Evaluation of Closed Needle Biopsy in 11 Consecutive Cases Am. J. Medicine. 84: 622, 1988.
120. PEARSON M.L.; JEREB J.A.; FIREDEN T.R; CRAWFORD J.L.; DAVIS H.; DOOLEY S.W. y JARVISR: NosocomialTransmission ofMultidrugresistant Mycobacterium tuberculosis: A Risk to Patients and Health Care Workers. Ann. Int. Med. 117, 191. 1992.
121. RAJASEKARAN S.; GOUNDARAPANDIAN S.: Progression of Kyphosis in tuberculosis of the spine treated by anterior arthrodesis. J. Bone Joint Surg.: 71-A: 1314, 1989.
122. RAHMANN.U.:AtypicaIFormsofSpinaITuberculosis. J. Bone Joint Surg.: 62-B: 162, 1980.
123. RAJESEKERANS.;SHANMUGSUNDARANT.K: Prediction of the Angle of Gibbus Deformity in Tuberculosis ofthe spine. J. Bone Joint Surg.: 69- A: 503,1987.
124. REIN v.C.F.; CLEMENTS C.J.; MANN J.M.: Human Immunodeficiency Virus Infection and routine childhood Immunisation. Lancet: 8560, 669, 1987.
125. RIEDER H.L.; SNIEDER D.E.; CANTHEU G.M.: Extrapulmonary tuberculosis in the United States. Am. Rev. Respir Dis.: 141: 347, 1990.
126. ROJAS L.; TORO J.: Tuberculosis en Chile. Enf. Resp. Cir. Tórax.: 1:4, 1985.
127. RUEDA-PEREZ G.: En el Centenario del descubrimiento del Mycobacterium tuberculosis por Roberto Koch:24 de marzo de 1982,Medicina: 6: 25, 1982.
128. RUEDA-PEREZ G.; TORRES C. A.; CHAVEZ G.: Actualización en tuberculosis: Medicina: 26: 2.
129. RUEDA-PEREZ G.: Estado actual de la TBC. Temas Médicos. ANM vol. 13. 1987.
130. RUEDA-PEREZ G.: Cirugía de la Tuberculosis Pulmonar. Primer Seminario de Epidemiología y Control de la Tuberculosis Memorias. Ibarra (Ecuador) 2-5julio 1991.
131. SARCARS.D.;RAVIKRISHNANP.;WOODBURY D.H.;CARSONJ.J.; DALEYK.:Gallium-67 Citrate Scanning-A new Adjunct in the Detection and Follow-up ofextrapulmonary tuberculosis. J. Nucl. Med. 20:833, 1979.
132. SARINHO E.; PONTINAL M.;DACOSTAM.;DA COSTA Ma.: Viragen tuberculinica Pos-vacinal. Com PPD derivado de BCG: OPS 11: 402, 1991.
133. SEULLY RE. Ced.)Case Records ofM.G.H. New England J. Med. 318, 306,1998.
134. SHAH P.; RAMAKANTANR: Tuberculosis of the patella.: British J. Radiol. 63: 363, 1990.
135. SHANNON F.B.; MOORE M.; HOUKOM J.A.; WACKER N.J.: Multifocal Cystic Tuberculosis ofBone. J. Bone Joint Surg.: 72-A 1089, 1990.
136. SHEA J.M.: Bilateral Tubercylous Osteomyelitis of Medial humeral Condyles. Infection Secondary to Cutaneous Inoculation. JAMA.: 247: 821,1982.
137. SINNOTT J.T.; CANCIO M.Z.; FRANKLE M.A.; GUSTKE K.; SPIEGEL P.G.: Tuberculous Osteomyelitis Marked by Concomitant Staphylococcal Infection. Arch. Intern. Med.: 150, 1865,1990.
138. SNIDER D.E.; RIEDER H.L.; CAMPSD.;BLOCH AB.; HAYDEN C.H.; SMITH M:H.D.: Tuberculosisin children: Pediat. Infect. Dis. J.: 7:271,1988.
139. SOLORZANOJ.J.; ALVAREZM.H.: Atención del enfermo tuberculoso a nivel comunitario en el estado de Chiapas. Méjico: O.S.P.: 111,432, 1991.
140. STAFFORD H.H.; WOODD.; GREGG P.J.: The in vitro release of Strepmycin from bone cemento J. Bone Joint Surg.: 72-B: 163, 1990
141. STEINER P.; RAOM.; MITCHELL M.; STEINER M.: Primary Drug-Resistant ofM. Tuberculosis to Rifampin. A Rev. Respir. Dis.: 134: 446,1986.
142. STRATHY G.M.; FITZGERALD R.H.: Total Hip ArthroplaE!ty in the Ankylosed hipo A ten-year follow-up. J. Bone Joint Surg.: 70-A 963, 1988.
143. STROEBEL A.B.; DANIEL T.M.; LAU J.H.K.; LERIG J.C. y RICHARDSSON H.: Serologic Diagnosis of Bone and Joint Tuberculosis by a Enzyme-Linked ImmunoselbentAssay. J. Infections Dis. 146:280, 1982.
144. SUNDERMAN G.;McDONALDR; MANIATIST. el al.: Tuberculosis as a manifesta tion ofthe acquired immunodeficiency syndrome CAIDS).JAMA 256, 1986.
145. TORRES C.A: Métodos diagnósticos complementarios en tuberculosis. Primer Seminario de Epidemiología y Control de tuberculosis. Ibarra, Ecuador. Julio 1991.
146. TORRES C.A: SIDAyTuberculosis. Primer Seminario de Epidemiología y Control de la tuberculosis. Ibarra, Ecuador. Julio 1991.
147. TORRES C.A: El pulmón en el paciente con SIDA: Actualizaciones en neumología. 95, Camacho F., Páez J.A, Awad C.E.: Hospital Santa Clara. Escuela Colombiana de Medicina. Publ. Zambón Co.Julio 1991.
148. VARELAC.:Tratamiento de la Tuberculosis según Programa. Primer Seminario de Epidemiología y Control de tuberculosis. Ibarra, Ecuador ,julio 1991.
149. USoDepartmentofHealth. Education, and Welfare, Public Health Service, Publication No. 638. Reported tuberculosis data, 1966, Washington, US Govermment Printing Office.
150. VILLARA: La tuberculosis en la década de 1990: O.P.s.: 111: 461, 1991.
151. VISHWARARKA G.K.; KHARE AK.: Amniotic arthroplasty for tuberculosis of the hipo J. Bone Joint. Surg.: 68-B: 68, 1986.
152. WILKINSON M.C.: Curetagge of the vertebral Disease in the Treatment of Spinal Caries. Proc. Roy. SocoMed. 43: 114, 1950.
153. WILKINSON M.C.: The treatment oftuberculosis of the spine by evacuation of the paravertebral abscess and curettage of the vertebral bodies. J. Bone Joint Surg.: 37-B: 382, 1955.
154. WHO. Weekly epidemiological record, Geneve: WHO, Jam 5, 1990.
155. WOLFGANG G.L.: Tuberculosis joint Infection’s followingtotal knee arthroplasy. Clin. Orthop. 201: 162,1985.
156. ZULUAGA L.; BETANCURT C.; ABAUNZA M.; LONDOÑO J.: Prevalecencia de tuberculosis y enfermedades respiratorias en personas mayores de 15 años de la Comuna Nororiental de Medellín Colombia, O.P.s.: 111: 406, 1991.
157. Secretaría de Salud de Bogotá. CUELLAR C., Comunicación personal. Mayo 1993.
158. COTRANSR;KUMARV.;ROBBINSS.L.:Robbins Pathology Basis ofDisease. 4th Ed. W.B. Saunders Co., Philadelphia 1989.
159. PATIÑO E.H.: Comunicación personal.