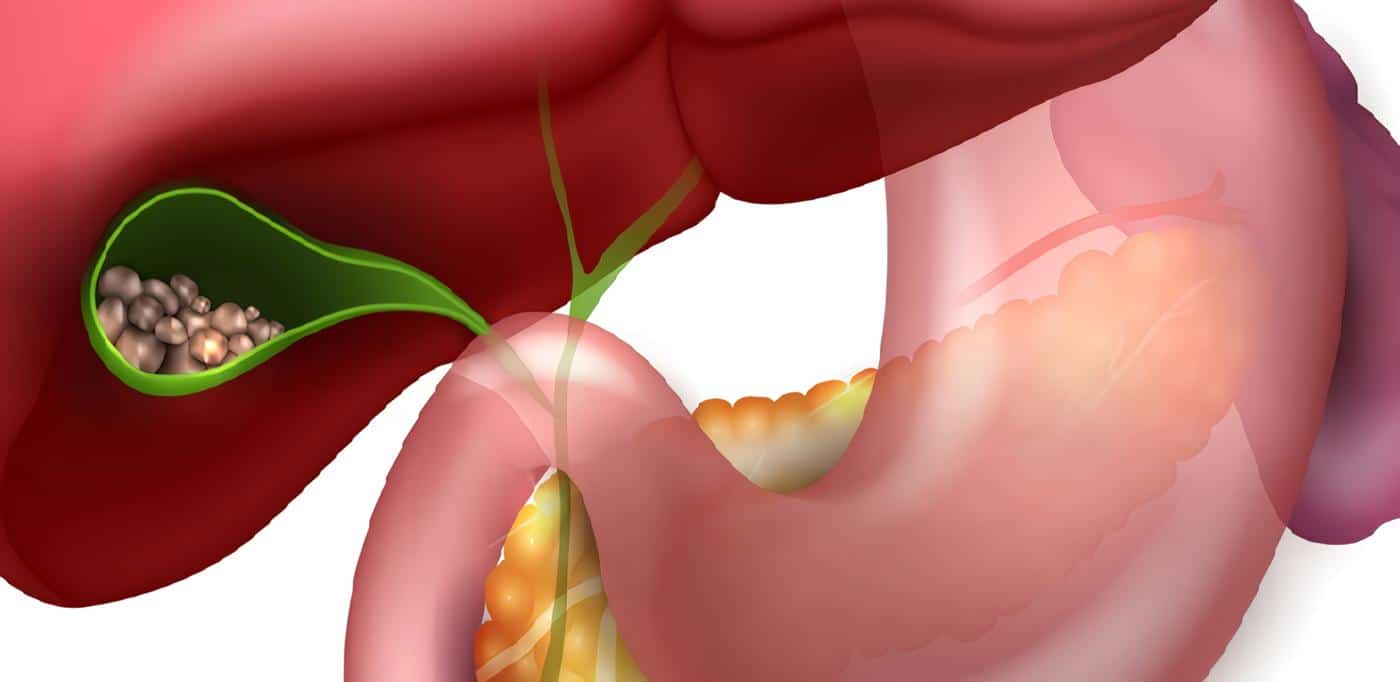
5. Colecistitis aguda
La mayoría de los pacientes con colecistitis aguda son tratados quirúrgicamente. Los pacientes con alto riesgo quirúrgico son un dilema. En ellos pueden realizarse drenajes vesiculares percutáneos guiados por ecografía.
Otra alternativa en estos últimos pacientes es el drenaje transpapilar de la vesícula por medio de endoprótesis o sondas nasovesiculares, en los sitios donde se cuente con el recurso y experiencia en CPRE. Se ha descrito el acceso a la vesícula en 86 a 90% de los casos (36-40). Evidencia nivel III.3.
Conclusiones
El drenaje transpapilar de la vesícula en pacientes con colecistitis aguda y alto riesgo quirúrgico es una alternativa a la cirugía o al drenaje percutáneo, donde existe el recurso de CPRE. Recomendación grado C.
Contraindicaciones
Aunque puede ser difícil y aún no se cuenta con parámetros objetivos para su selección, el juicio clínico puede ayudar en pacientes terminales, con una supervivencia esperada menor de un mes, en los cuales es muy poco el beneficio que obtendrían de un drenaje endoscópico (8). Aquellos pacientes con tumores proximales de tercer grado, con compromiso de múltiples ramas intrahepáticas, es muy poco el beneficio que reciben de una prótesis (21).
La coagulopatía, la hipoxemia y el mal estado general, en especial en los casos de colangitis, son contraindicaciones relativas. Con respecto a la coagulopatía, si el paciente da tiempo se puede corregir con vitamina K o transfusión de plaquetas.
Pero de ser necesario un procedimiento urgente, éste se puede llevar a cabo colocando la prótesis o la sonda naso-biliar sin realizar una papilotomía. En pacientes en malas condiciones, el concurso de un anestesiólogo para ayudar en el control y la monitorización del paciente es de mucha ayuda. El procedimiento en estos pacientes puede realizarse con una mínima o con ninguna sedación, en forma rápida.
IV. Equipo
A. General:
Sala de rayos X con fluoroscopio
Duodenoscopio con canal de 4,2 mm
Ayudante entrenado
Electrobisturí
Fuente de oxígeno
Monitorización: pulsoxímetro
B. Accesorios:
Papilótomo convencional
Papilótomo de precorte
Dilatador – catéter universal – catéter guía con marcas radioopacas
Guía de teflón 0,35
Guía hidrofílica
Endoprótesis de diferente diámetro, 7 a 10F.
Posicionador de endoprótesis
C. Opcional:
Catéteres dilatadores de diferente diámetro
Balón dilatador hidrostático biliar, 6 a 10mm
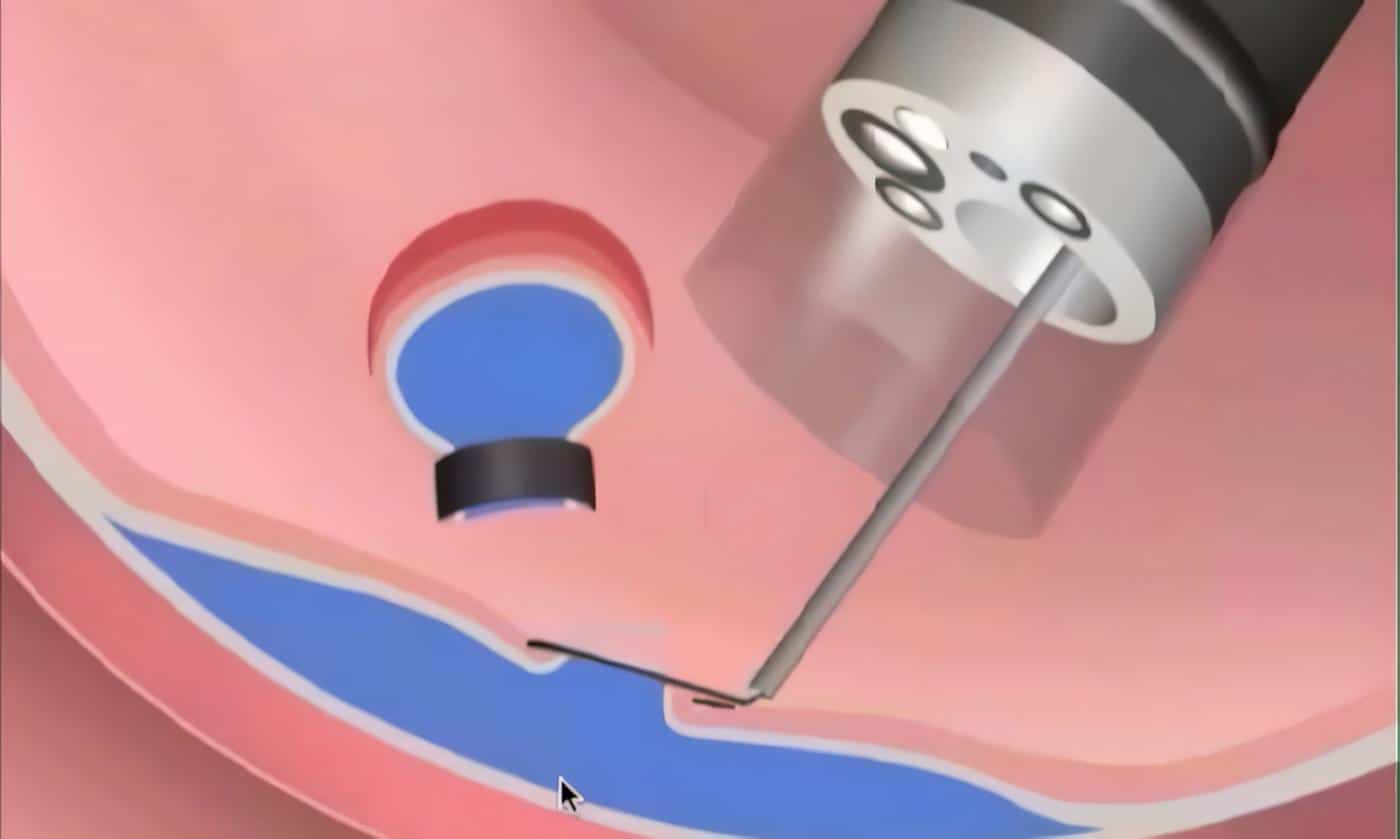
V. Técnica
Brevemente, el procedimiento se lleva a cabo bajo sedación, con antibióticoterapia profiláctica para los pacientes obstruidos (41). Se canaliza la vía biliar delineando la obstrucción.
Se manipula una guía a través de la estenosis, de ser necesario se utiliza una guía hidrofílica, pasando luego sobre ésta un catéter dilatador. En este momento, se contrasta el árbol biliar proximal sin inyectar medio de contraste a presión. Entonces, se pueden tomar las muestras para citología.
Sobre la guía de teflón se coloca la prótesis o el sistema catéter-guía prótesis, la cual se empuja con el posicionador de endoprótesis de color diferente al de ésta. Las prótesis deben medir 2 a 3 cm más que la longitud estimada de la estenosis, y finalmente deben quedar protruyendo no más de un cm de la papila.
Las prótesis pueden colocarse sin papilotomía, aunque ésta facilita la inserción de una segunda prótesis en casos de tumores proximales que obstruyen la bifurcación. Cuando se utiliza una prótesis 10 French sin papilotomía, se han descrito casos de pancreatitis posterior al procedimiento en pacientes con tumores proximales, por lo que en estos casos es aconsejable practicarla (42).
VI. Bibliografía
- 1. Soehendra N, Reyders-Federix. Palliative Bile Duct Drainage – A new endoscopic method of introducing a transpapillary drain. Endoscopy 1980; 12: 8-11.
- 2. Speer AG, Cotton PB, Russel RC, et al. Randomised trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Lancet 1987; 2(8550): 57-62.
- 3. Andersen JR, Sorensen SM, Kruse A, et al. Randomised trial of endoscopic endoprosthesis versus operative bypass in malignant obstructive jaundice. Gut 1989; 30: 1132-35.
- 4. Smith AC, Dowsett JF, Russell RCG, Hatfield ARW, Cotton PB. Randomised trial of endoscopic stenting ver sus surgical bypass in malignant low bileduct obstruction. Lancet 1994; 344: 1655-60.
- 5. Van Den Bosch RP, Van der Schelling GP, Klinkenbijl JHG, et al. Guidelines for the applications of surgery and endoprostheses in the palliation of obstructive jaundice in advanced cancer of the pancreas. Ann Surg 1994; 219(1): 18-23.
- 6. Lai EC, Mok FP, Fan ST, et al. Preoperative endoscopic drainage for malignant obstructive jaundice. Br J Surg 1994; 81(8): 1195-8.
- 7. Ballinger AB, McHugh M, Catnach SM, et al. Symptom relief and quality of life after stenting for malignant bile duct obstruction. Gut 1994; 35: 467-70.
- 8. Sherman S, Lehman G, Earle D, et al. Endoscopic palliation of malignant bile duct obstruction: improvement in quality of life. Gastrointest Endosc 1997; 45(4): AB147.
- 9. Speer AG, Cotton PB, MacRae KD. Endoscopic Management of Malignant Biliary Obstruction: Stents of 10 French gauge are preferable to Stents of 8 French Gauge. Gastrointest Endosc 1988; 34(5): 412-7.
- 10. Pedersen FM. Endoscopic Management of Malignant Biliary Obstruction. Is Stent Size of 10 French Gauge better than 7 French Gauge? Scand J Gastroenterol 1993; 28(2): 185-189.
- 11. Meyerson SM, Greenen JE, Catalano MF, et al. “Tanembaum” Teflon Stents vs Traditional Polyethylene Stents for Treatment of Malignant Biliary Strictures: A multicenter Prospective Randomized Trial. Gastrointest Endosc 1998; 47(4): AB122.
- 12. Sung JJY, Sidney Chung SC, Chi-Ping Tsui, et al. Omitting Side-Holes in Biliary Stents does not Improve Drainage of the Obstructed Biliary System: A Prospective Randomised Trial. Gastrointest Endosc 1994; 40: 321-5.
- 13. Van Berkel AM, Boland C, Rdekop WK, et al. A Prospective Randomised Trial of Teflon Versus Polyethylene Stents for Distal Malignant Biliary Obstruction. Endoscopy 1998; 30(8): 681-86.
- 14. Prat F, Chapat O, Ducot B, et al. A Randomized Trial of Endoscopic Drainage Methods for Inoperable Malignant Strictures of the Common Bile Duct. Gastrointest Endosc 1998; 47(1): 1-7.
- 15. Rossi P, Bezzi M, Rossi M, et al. Metallic Stents in Malignant Biliary Obstructions: Results of a Multicenter European Study of 240 Patients. J Vasc Interv Radiol 1994; 5(2): 279-85.
- 16. Shim CS, Lee YH, Cho YD, et al. Preliminary Results of a New Covered Biliary Metal Stent for Malignant Biliary Obstruction. Endoscopy 1998; 30: 345-50.
- 17. Born P, Neuhaus H, Rösch T, et al. lnitial Experience with a new, partially covered Wallstent for Malignant Biliary Obstruction. Endoscopy 1996; 699-702.
- 18. Prat F, Chapat AO, Ducot AB, et al. Predictive factors for survival of patients with inoperable malignant distal biliary strictrures: A practical management guideline. Gut 1998; 42: 76-80.
- 19. Chang WH, Kortan P, Haber GB. Outcome in patients with bifurcation tumors who undergo unilateral versus bilateral hepatic duct drainage. Gastrointest Endosc 1998; 47(5): 354-62.
- 20. Polydorou AA, Caims SR, Cowsett JF, et al. Palliation of Proximal Malignant Biliary Obstruction by Endoscopic Endoprosthesis Insertion. Gut 1991; 32: 685-89.
- 21. Ducreux M, Liguory C, Lefebvre JF, et al. Management of Malignant Hilar Biliary Obstruction by Endoscopy. Results and Prognostic Factors. Dig Dis Sci 1992; 37(5): 778-83.
- 22. Gordon RL, Ring EJ, LaBerge JM, Doehrty MM. Malignant Biliary Obstruction: Treatment with Expandable Metallic Stents – Follow-up of 50 Consecutive Patients. Radiology 1992; 182(3): 698-701.
- 23. Cheung KL, Lai EC. Endoscopic Stenting for Malignant Biliary Obstruction. Arch Surg 1995; 130(2): 204-7.
- 24. Pereira-Lima JC, Jakobs R, Maier M, et al. Endoscopic Stenting in Obstructive Jaundice due to liver Metastases: Does it have a Benefit for the Patient? Hepatogastrienterology 1996; 43(10): 944-8.
- 25. De Masi E, Fiori E, Lamazza A, et al. Endoscopy in the Treatment of Benign Biliary Strictures. Ital J Gastroenterol Hepatol 1998; 30(1): 91-5.
- 26. Davids PHP, Tanka AKF, Rauws EAJ, et al. Benign Biliary Strictures. Surgery or Endoscopy? Ann Surg 1993; 217(3): 237-43.
- 27. Du Vall A, Haber G, Kortan P, et al. Long Term Follow-up of Endoscopic Stenting for Benign Postoperative Bile Duct Strictures. Gastrointest Endosc 1997; 45(4): AB129.
- 28. Davids PH, Rauws EA, Tygat GN, Huibregstse K. Postoperative Bile Leakage: Endoscopic Management. Gut 1992; 33(8): 1118-22.
- 29. Liguory C, Vitale GC, Lefebre JF, Bonnel D, Comud F. Endoscopic Treatment of Postoperative Biliary Fistulae. Surgery 1991; 110(4): 779-83.
- 30. Binmoeller KF, Daton RM, Shneidaman R. Endoscopic Management of Postoperative Biliary Leaks: Review of 77 Cases and Report of Two Cases with Biloma Formation. Am J Gastroenterol 1991; 86(2): 227-31.
- 31. Seitz U, Bapaye A, Bohnacker S, et al. Advances in Therapeutic Endoscopic Treatment of Common Bile Duct Stones. World J Surg 1998; 22(11): 1133-44.
- 32. Chopra KB, Peters RA, O’Toole PA, et al. Randomised Study of Endoscopic Biliary Endoprosthesis Versus Duct Clearance fo Bile Duct Stones in High Risk Patients. Lancet 1996; 348(9030): 791-3.
- 33. Maxton DG, Tweedle DE, Martin DF. Retained Common bile Duct Stones After Endoscopic Sphincterotomy: Temporary and longterm Treatment with Biliary Stenting. Gut 1995; 36(3): 446-9.
- 34. Bergman JJ, Rauws EA, Tijssen JG, Tygat GN, Huibregstse K. Biliary Endoprotheses in Elderly Patients with Endoscopically Irretrievable Common Bile Duct Stones: Report on 117 Patients. Gastrointest Endosc 1995; 42(3): 195-201.
- 35. Lai ECS, Mok FPT, Tan ESY, et al. Endoscopic Biliary Drainage for Sever Acute Cholangitis. New Eng J Med 1992; 326(24): 1582-86.
- 36. Kalloo AN, Thuluvath PJ, Pasrricha PJ. Treatment of High Risk Patients with Symptomatic Cholelithiasis by Endoscopic Gallbladder Stenting. Gastrointest Endosc 1994; 40: 608-10.
- 37. Soehendra N, Schulz H, Nam V.Ch, et al. ESWL and Gallstone Dissolution with MTBE via a Naso-Vesicular Cateheter. Endoscopy 1990; 22: 176-9.
- 38. Fumas R, Caroli-Bosc FX, Demarquay JF, et al. Acute Inoperable Cholecystitis Treated by Endoscopic Naso-Vesicular Drainage. Gastroenterol Clin Biol 1997; 21(11): 854-8.
- 39. Tamada K, Seki H, Sato K, et al. Efficacy of Endoscopic Retrograde Cholecystoendosprosthesis (ERCCE) for Cholecystitis. Endoscopy 1991; 23(1): 2-3.
- 40. Feretis C, Apostolidis N, Mallas E, Manouras A, Papdimitriou J. Endoscopic Drainage of Acute Obstructive Cholecystitis in Patients with Increased Operative Risk. Endoscopy 1993; 25(6): 392-5.
- 41. Niederau C, Pohlmann U, Lubke H, Thomas L. Prophylactic Antibiotic Treatment in Therapeutic or Complicated Diagnostic ERCP: Results of a Randomized Controlled Clinicall Study. Gastrointest Endosc 1994; 40: 533-3.
- 42. Tamasky PR, Cunningham JT, Hawes RH, et al. Transpapillary Stenting of Proximal Biliary Strictures: Does Biliary Sphincterotomy Reduce the Risk of Postprocedure Pancreatitis? Gastrointest Endosc 1997; 45(1): 46-51.