En el presente estudio se obtuvieron una sensibilidad del 80,0 % y una especificidad del 98,7 % para la cACAF, valores similares a los reportados en la literatura científica 38-46 y superiores a los encontrados por nuestro grupo en una evaluación retrospectiva, en la cual se reportó una sensibilidad de 35,2 % 12. Por lo tanto, con base en los presentes hallazgos, se puede sugerir que la implementación de la guía ecográfica en la obtención de las muestras citológicas, la disminución de la frecuencia de extendidos insatisfactorios e indeterminados y la interpretación de dichos extendidos por personal entrenado, pueden aumentar en forma significativa el rendimiento de esta prueba 47.
Tabla 3.
Correlación entre las categorías de diagnóstico hecho mediante biopsia por congelación y diagnóstico histopatológico de los especímenes en estudio (p=0,000)
 HPM: histología positiva para neoplasia maligna; HNM: histología negativa para neoplasia maligna; BCPM: biopsia por congelación positiva para neoplasia maligna; BCNM: biopsia por congelación negativa para neoplasia maligna; CP: carcinoma papilar; CF: carcinoma folicular; CA: carcinoma anaplásico; CM: carcinoma medular; BSA: bocio coloide sin cambios adenomatosos; BCA: bocio coloide con cambios adenomatosos; TH: tiroiditis linfocítica crónica; AF: adenoma folicular.
HPM: histología positiva para neoplasia maligna; HNM: histología negativa para neoplasia maligna; BCPM: biopsia por congelación positiva para neoplasia maligna; BCNM: biopsia por congelación negativa para neoplasia maligna; CP: carcinoma papilar; CF: carcinoma folicular; CA: carcinoma anaplásico; CM: carcinoma medular; BSA: bocio coloide sin cambios adenomatosos; BCA: bocio coloide con cambios adenomatosos; TH: tiroiditis linfocítica crónica; AF: adenoma folicular.
Tabla 4.
Distribución de los diagnósticos clínicos definitivos de las enfermedades quirúrgicas de la glándula tiroides en la E.S.E. Hospital Universitario del Caribe, durante el periodo 2014-2015
 EH: enfermedad de Hashimoto; BMS: bocio multinodular simple.
EH: enfermedad de Hashimoto; BMS: bocio multinodular simple.
Durante el año de seguimiento, para la cACAF solo se encontraron dos falsos negativos (2,4 %) y un falso positivo (1,2 %). La imprecisión en un caso falso positivo y un caso falso negativo, correspondientes a un bocio sin cambios adenomatosos clasificado como Bethesda V y a un carcinoma papilar clasificado como Bethesda II, se asoció a la aspiración de nódulos menores de 10 mm, en el contexto de un bocio multinodular simple y una enfermedad de Hashimoto, respectivamente. Por otro parte, el caso falso negativo restante, correspondiente a un carcinoma folicular clasificado citológicamente como Bethesda II, puede asociarse con la baja sensibilidad de la cACAF en el diagnóstico de las neoplasias foliculares, encontrada en estudios realizados por nuestro grupo, y puede justificarse por las similitudes citológicas existentes entre estas neoplasias y los bocios con cambios adenomatosos 48. Sin embargo, ninguno de los casos anteriormente expuestos fue sometido a reintervenciones o procedimientos quirúrgicos innecesarios gracias a la biopsia por congelación, lo que respalda, pese a estudios que aseguran lo contrario 49,50, el impacto de esta prueba en el manejo intraoperatorio de este grupo de pacientes.
Tabla 5.
Comparación entre el rendimiento de la citología obtenida mediante aspiración con aguja fina y el de la biopsia por congelación, en el diagnóstico de las neoplasias malignas de la glándula tiroides (k=0,952)
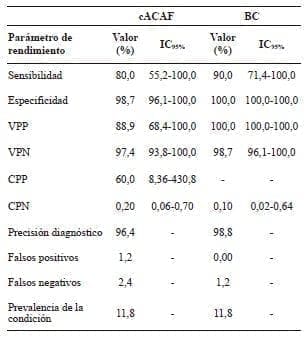 cACAF: citología por aspiración con aguja fina; BC: biopsia por congelación; VPP: valor predictivo positivo; VPN: valor predictivo negativo; CPP: cociente de probabilidad positivo; CPN: cociente de probabilidad positivo.
cACAF: citología por aspiración con aguja fina; BC: biopsia por congelación; VPP: valor predictivo positivo; VPN: valor predictivo negativo; CPP: cociente de probabilidad positivo; CPN: cociente de probabilidad positivo.
Con respecto a la biopsia por congelación, se reportó una sensibilidad de 90,0 % y una especificidad de 100,0 % en el diagnóstico de las neoplasias malignas, parámetros superiores a los reportados en la literatura científica 38,43,46, excluyendo aquellos estudios en los cuales se evalúa su rendimiento en el manejo de los pacientes con extendidos citológicos sospechosos de neoplasia folicular, en los cuales la aplicabilidad de la biopsia por congelación continúa siendo un reto 51,52.
En nuestro seguimiento, se encontró un único caso falso negativo (1,2 %), correspondiente a un carcinoma papilar. El resultado negativo del estudio se explicó porque la lesión no se encontraba en el espécimen quirúrgico del cual se realizaron los cortes por congelación. No obstante, por las características clínicas del paciente y el aspecto macroscópico del espécimen restante, se decidió practicar una tiroidectomía total más vaciamiento central, encontrándose posteriormente la lesión maligna en el estudio anatomo-patológico.
Conclusión
Nuestros resultados sustentan que la cACAF continúa siendo la mejor herramienta en el abordaje inicial del paciente con enfermedad nodular de la glándula tiroides. La excelente concordancia de la cACAF y la biopsia por congelación en el diagnóstico de las neoplasias malignas de la glándula tiroides (k=0,952), no justifica el uso rutinario de la biopsia por congelación en pacientes con diagnósticos citológicos benignos y malignos; sin embargo, su uso en el manejo intraoperatorio de los pacientes con citologías sospechosas de neoplasia maligna, podría disminuir significativamente la frecuencia de falsos positivos.
Conflictos de interés
Los autores no manifiestan conflictos de intereses.
Comparison between fine needle aspiration cytology and frozen section biopsy in the diagnosis of malignant neoplasms of the thyroid gland: a prospective study
Abstract
Introduction: Fine-needle aspiration cytology (FNAC) and frozen section (FS) are currently considered cornerstones in the diagnosis of thyroid gland nodular lesions. The main goal of the present study is to prospectively compare the performance of FNAC and FS in the diagnosis of malignant neoplasms of the thyroid at the E.S.E Hospital Universitario del Caribe, Cartagena, Colombia.
Methods: Between April 2014 and June 2015, FNAC and FS were obtained in a prospective way by a radiologist and a neck surgeon, respectively. The results of the FNAC and the FS were compared with the pathology report. The following performance parameters were included: sensitivity, specificity, positive predictive value, negative predictive value, diagnostic accuracy, false positive and false negative percentage. The kappa index for concordance was used to compare the performance of FNAC and FS.
Results: The population study consisted of 85 patients, 92,9% female, with average age 45,3 ± 14,7 years. The following performance parameters for FNAC and FS were determined: sensitivity 80,0% / 90,0%; specificity, 98,7% / 100,0%; positive predictive value 88,9% / 100,0%; negative predictive value, 97,4% / 98,7%; diagnostic accuracy 96,5% / 98,8%; false positives percentage, 1,2% / 0.0%, false negatives percentage, 2,4% / 1,2% and kappa index for concordance of 0.952.
Conclusion: FNAC and the FS have a concordance index of 0.952 in the diagnosis of thyroid malignant neoplasms. These results do not suggest the routine use of FS, however they do suggest that the use of FS in the intraoperative management of patients with cytologic diagnosis of “suspicious for malignancy” lower even more the frequency of false positives.
Key words: thyroid neoplasms; biopsy, fine-needle; frozen sections; cytology; diagnosis; sensitivity and specificity.
Referencias
1. Hamberger B, Gharib H, Melton LJ, Goellner JR, Zinsmeister AR. Fine-needle aspiration biopsy of thyroid nodules: Impact on thyroid practice and cost of care. Am J Med. 1982;73:381-4.
2. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167-214.
3. Leenhardt L, Erdogan MF, Hegedus L, Mandel SJ, Paschke R, Rago T, et al. European Thyroid Association for cervical ultrasound scan and ultrasound-guided techniques in the postoperative management of patients with thyroid cancer. Eur Thyroid J. 2013;2:147-59.
4. NaÏm C, Karam R, Eddé D. Ultrasound-guided fine-needle aspiration biopsy of the thyroid: Methods to decrease the rate of unsatisfactory biopsies in the absence of an on-site pathologist. Can Assoc Radiol J. 2013;64:220-5.
5. Harvey AM, Mody DR, Amrikachi M. Thyroid fine-needle aspiration reporting rates and outcomes before and after Bethesda implementation within a combined academic and community hospital system. Arch Pathol Lab Med. 2013;137:1664-8.
6. Gharib H, Goellner JR. Fine-needle aspiration biopsy of the thyroid: An appraisal. Ann Intern Med. 1993;118:282-9.
7. Gharib H, Goellner JR, Johnson DA. Fine-needle aspiration cytology of the thyroid gland: A 12-year experience with 11,000 biopsies. Clin Lab Med. 1993;13:699-709.
8. Gharib H, Goellner JR. Fine-needle aspiration biopsy of thyroid nodules. Endocr Pract. 1995;1:410-7.
9. Pedroza A. Manejo del nódulo tiroideo: revisión de la literatura. Rev Colomb Cir. 2008;43:257-71.
10. Román A, Restrepo L, Alzate C, Vélez A, Gutiérrez J. Nódulo tiroideo, enfoque y manejo. Revisión de la literatura. Iatreia. 2013;26:197-206.
11. Melo-Uribe MA, Sanabria Á, Romero-Rojas A, Pérez G,
Vargas EJ, Abaúnza MC, et al. The Bethesda System for Reporting Thyroid Cytopathology in Colombia: Correlation with histopathological diagnoses in oncology and non-oncology institutions. J Cytol. 2015;32:12-6.
12. Herrera F, Castañeda S, Contreras S, Fernández A, Pérez E. Rendimiento diagnóstico de la citología por aspiración con aguja fina en pacientes con nódulo tiroideo en la E.S.E. Hospital Universitario del Caribe. Rev Colomb Cir. 2014;29:313-8.
13. Jo VY, Stelow ES, Dustin SM, Hanley KZ. Malignancy risk for fine needle aspiration of thyroid lesions according to the Bethesda System for Reporting Thyroid Cytopathology. Am J Clin Pathol. 2010;134:450-6.
14. Yassa L, Cibas ES, Benson CB, Frates MC, Doubilet PM, Gawande AA, et al. Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer 2007;111:508-16.
15. Yang J, Schnadig V, Logrono R, Wasserman PG. Fine-needle aspiration of thyroid nodules: A study of 4703 patients with histologic and clinical correlations. Cancer. 2007;111:306-15.
16. Nayar R, Ivanovic M. The indeterminate thyroid fine‑needle aspiration: Experience from an academic center using terminology similar to that proposed in the 2007 National Cancer Institute thyroid fine needle aspiration state of the science conference. Cancer 2009;117:195-202.
17. Mondal SK, Sinha S, Basak B, Roy DN, Sinha SK. The Bethesda system for reporting thyroid fine needle aspirates: A cytologic study with histologic follow-up. J Cytol. 2013;30:94-9.
18. Antic T, Taxy JB. Thyroid frozen section: Supplementary or unnecesary. Am J Surg Pathol. 2013;37:282-6.
19. Cibas ES, Syed ZA, Ali SZ. NCI Thyroid FNA State of the Science Conference. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009;132:658-65.
20. Bakhos R, Selvaggi SM, DeJong S, Gordon DL, Pitale SU, Herrmann M, et al. Fine-needle aspiration of the thyroid: Rate and causes of cytohistopathologic discordance. Diagn Cytopathol. 2000;23:233-7.
21. Amrikachi M, Ramzy I, Rubenfeld S, Wheeler TM. Accuracy of fine-needle aspiration of thyroid. Arch Pathol Lab Med. 2001;125:484-8.
22. Khan I, Naz S, Mehmood A, Aziz N. Diagnostic accuracy of fine needle aspiration of thyroid nodule verses biopsy in thyroid lesions. J Ayub Med Coll Abbottabad. 2000;22:174-81.
23. Morgan JL, Serpell JW, Cheng MS. Fine-needle aspiration cytology of thyroid nodules: How useful is it? ANZ J Surg. 2003;73:480-3.
24. Ko HM, Jhu IK, Yang SH, Lee JH, Nam JH, Juhng SW, et al. Clinico-pathologic analysis of fine needle aspiration cytology of the thyroid. A review of 1,613 cases and correlation with histopathologic diagnoses. Acta Cytol. 2003;47:727-32.
25. Jogai S, Al-Jassar A, Temmim L, Dey P, Adesina AO, Amanguno HG. Fine needle aspiration cytology of the thyroid: A cytohistologic study with evaluation of discordant cases. Acta Cytol. 2005;49:483-8.
26. Cai XJ, Valiyaparambath N, Nixon P, Waghorn A, Giles T, Helliwell T. Ultrasound-guided fine needle aspiration cytology in the diagnosis and management of thyroid nodules. Cytopathology. 2006;17:251-6.
27. Chih-En T, Chang-Kuo W, Chin-Sung K, Shih-Tang Y, Pin- Fan C, Wei-Cheng L, et al. Fine needle aspiration cytology of thyroid nodules: Evaluation of diagnostic accuracy. Tzu Chi Med J. 2008;20:296-303.
28. Arrechedera-Pacheco C, Oviedo N, Linares Y, Sanabria E, Canozo L. La punción con aguja fina método de estudio diagnóstico en nódulos de la glándula tiroides. Rev Venez Oncol. 2009;21:77-84.
29. Seningen JL, Nassar A, Henry MR. Correlation of thyroid nodule fine-needle aspiration cytology with corresponding histology at Mayo Clinic, 2001-2007: An institutional experience of 1,945 cases. Diagn Cytopathol. 2012;40(Suppl.1):E27-32.
30. Tariq M, Zafar-Iqbal M, Zulifqar-Ali M, Anwar-Ch M, Sulman- Khan R, Irum S. FNAC of thyroid nodule: Diagnostic accuracy of fine needle aspiration cytology (FNAC). Professional MedJ. 2010;17:589-97.
31. Piana S, Frasoldati A, Ferrari M, Valcavi R, Froio E, Barbieri V, et al. Is a five-category reporting scheme for thyroid fine needle aspiration cytology accurate? Experience of over 18,000 FNAs reported at the same institution during 1998-2007. Cytopathology. 2011;22:164-73.
32. Sellami M, Tababi S, Mamy J, Zainine R, Charfi A, Beltaief N, et al. Interest of fine-needle aspiration cytology in thyroid nodule. Eur Ann Otorhinolaryngol Head Neck Dis. 2011;128:159-64.
33. Jammah A. Evaluation of the accuracy of fine-needle aspiration cytology in the diagnosis of thyroid nodules: A retrospective analysis of data from a tertiary care hospital in Saudi Arabia. Turk Jem. 2012;16:30-3.
34. Cheng MS, Morgan JL, Serpell JW. Does frozen section have a role in the operative management of thyroid nodules. ANZ J Surg. 2002;72:570-2.
35. Wong Z, Mothu C, Craik J, Carter J, Harman CR. Role of intraoperative frozen section in the management of thyroid nodules. ANZ J Surg. 2004;74:1052-5.
36. Huber GF, Dzieguelewski P, Matheus TW, Warshawski SJ, Kmat LM, Faris P, et al. Intraoperative frozen-section analysis for thyroid nodules: A step toward clarity or confusión? Arch Otolaryngol Head Neck Surg. 2007;133:874-81.
37. Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwing LM, et al. The STARD statement for the reporting studies of diagnostic accuracy: Explanation and elaboration. Ann Intern Med. 2003;138:W1-12.
38. Prades JM, Querat C, Dumollard JM, Richard C, Gavid M, Timoshenko AA, et al. Thyroid nodule surgery: Predictive diagnostic value of fine-needle aspiration cytology and frozen section. Eur Ann Otorhinolaryngol Head Neck Dis. 2013;130:195-9.
39. Knezevic-Usaj S, Eri Z, Panjkovic M, Klem I, Petrovic T, Ivkovic-Kapicl T, et al. Diagnostic relevance of the fine needle aspiration cytology in nodular thyroid lesions. Vojnosanit Pregl. 2012;69:555-61.
40. Haberal AN, Toru S, Özen Ö, Arat Z, Bilezikci B. Diagnostic pitfalls in the evaluation of fine needle aspiration cytology of the thyroid: Correlation with histopathology in 260 cases. Cytopathology. 2009;20:103-8.
41. Bista M, Toran KC, Regmi D, Maharjan M, Kafle P, Shrestha S. Diagnostic accuracy of fine needle aspiration cytology in thyroid swellings. J Nepal Health Res Counc 2011;9:14-6.
42. Mandal S, Bardman D, Mukerjee A, Mukherjee D, Saha J, Sinhas R. Fine needle aspiration cytology of thyroid nodules: Evaluation of its role in diagnosis and management. J Indian Med Assoc. 2001;109:258-61.
43. Kumar M, Potekar R, Yelikar BR, Patil V, Karigoudar M, Pande P. Diagnostic accuracy of frozen section in comparison with fine needle aspiration cytology in thyroid: A prospective study. Iran J Pathol. 2013;8:219-26.
44. Rodríguez Z, Dorimain PC, Falcon GC, Mustelier HL. Diagnóstico de los nódulos de tiroides mediante estudio citológico mediante punción y aspiración con aguja fina. MEDISAN. 2013;17:1.
45. Gelincik I. The comparison of fine needle aspiration cytology and histopathology results in hypoactive solitary nodules. Firat Tip Dergisi. 2013;1882:83-7.
46. Almeida JP, Couto SD, Rocha RP, Pfuetzenreiter EG, Devivitis RA. The role of intraoperative frozen sections for thyroid nodules. Braz J Otorhinolaryngol. 2009;75:256-60.
47. Naïm C, Karam R, Eddé D. Ultrasound-guided fine-needle aspiration biopsy of the thyroid: Methods to decrease the rate of unsatisfactory biopsies in the absence of an on-site pathologist. Can Assoc Radiol J. 2013;6483:220-5.
48. Herrera F, Redondo K, Osorio C, Grice J, Fernández A. Utilidad de la citología obtenida mediante aspiración con aguja fina en el diagnóstico de las neoplasias foliculares de la glándula tiroides en la E.S.E. Hospital Universitario del Caribe: un estudio retrospectivo. Rev Colomb Cir. 2015;30:12-7.
49. Cetin B, Aslan S, Hatiboglu C, Babacan B, Onder A, Celik A, et al. Frozen section in thyroid surgery: Is it a necessity? Can J Surg. 2004;47:29-33.
50. Kahmke R, Lee WT, Puscas L, Scher RL, Shealy MJ, Burch WM, et al. Utility of intraoperative frozen sections during thyroid surgery. Intern J Otorlaryn. 2013; ID 496138. http://dx.doi.org/10.1155/2013/496138.
51. Leteurte E, Leroy X, Pattou F, Wacrenier A, Carnaille B, Proye C, et al. Why do frozen sections have limited value in encapsulated or minimally invasive follicular carcinoma of the thyroid? Am J Clin Pathol. 2001;115:370-4.
52. Chen H, Nicol TL, Udelsman R. Follicular lesions of the thyroid. Does frozen section evaluation alter operative management. Ann Surg. 1995;222:101-6.
Correspondencia:
Grupo de Investigación Scalpellum
cosorioc@gruposcalpellum.com
Cartagena, Colombia